DF - NO!
The article is anti-vaxxer propaganda
It is pictured BS - IMHO!
Some of the article is reasonable - criticism of eh Ferguson model has been accepted widely in eh medical /scientific community. The model was developed very early in teh pandemic - and has proved to be inaccurate.
Appended - a scholarly article on the 1918 Spanish influenza epidemic and vaccines.
I urge the Forum posters to read this.
Thank you!\
Public Health Rep. 2010; 125(Suppl 3): 27–36.
doi:
10.1177/00333549101250S306
PMCID: PMC2862332
PMID:
20568567
The State of Science, Microbiology, and Vaccines Circa 1918
John M. Eyler, PhDa
Author information Copyright and License information Disclaimer
This article has been
cited by other articles in PMC.
Go to:
SYNOPSIS
The influenza pandemic of 1918–1919 dramatically altered biomedical knowledge of the disease. At its onset, the foundation of scientific knowledge was information collected during the previous major pandemic of 1889–1890. The work of Otto Leichtenstern, first published in 1896, described the major epidemiological and pathological features of pandemic influenza and was cited extensively over the next two decades. Richard Pfeiffer announced in 1892 and 1893 that he had discovered influenza's cause. Pfeiffer's bacillus (
Bacillus influenzae) was a major focus of attention and some controversy between 1892 and 1920. The role this organism or these organisms played in influenza dominated medical discussion during the great pandemic.
Many vaccines were developed and used during the 1918–1919 pandemic. The medical literature was full of contradictory claims of their success; there was apparently no consensus on how to judge the reported results of these vaccine trials. The result of the vaccine controversy was both a further waning of confidence in Pfeiffer's bacillus as the agent of influenza and the emergence of an early set of criteria for valid vaccine trials.
When the great influenza pandemic of 1918–1919 began, the most important sources of knowledge about epidemic influenza were studies conducted during and immediately following the previous pandemic, that of 1889–1990. The 1889–1890 influenza pandemic was the first to occur in the Western world after the pandemic of 1848–1849. That meant that it was the first to have taken place since more prosperous nation states had created active, professional health departments and systems of vital statistics, and the first to be studied using the methods of modern pathology and bacteriology. The 1889–1890 pandemic generated a very large literary output and two particularly important biomedical syntheses. In 1891, Franklin Parsons, a member of the Medical Department of the Local Government Board in London, published a 300-page report on the pandemic based on surveys of all sanitary districts in England and Wales and on local studies in selected areas.
1 Five years later, drawing on continental, especially German, scientific and clinical literature, Otto Leichtenstern published the definitive scientific study of influenza in Hermann Northnagel's multi-volume handbook of special pathology.
2,
3 These two major works, particularly Leichtenstern's, were the well from which American authors of medical textbooks and reference works, such as William Osler and Frederick Lord, would draw for the next two decades and the standards against which medical authorities would judge their observations and conclusions during the next great pandemic.
4–
6
It says volumes about the rudimentary state of scientific knowledge of influenza in the early 1890s that the most important and lasting conclusion of these two seminal works was that influenza was a specific, communicable disease.
1,
3 (p. 51–3, 70–102) (p. 554–64, 573–5) It did spread very rapidly, more rapidly than any other known communicable disease, and it produced explosive local outbreaks. However, it never arose spontaneously, nor did it travel faster than humans travel. Close investigation easily debunked accounts of outbreaks occurring without precursor cases or in places without contact with infected individuals. Furthermore, isolated populations, such as those within prisons in heavily infected cities, sometimes escaped entirely. Although influenza occurred more often in winter and spring months, the pandemic struck in all latitudes of both hemispheres, at all altitudes inhabited by humans, and in all climates. It was clearly not caused by overt climatic or environmental factors. A serious influenza epidemic was seldom a solo event. A major epidemic was often followed within months by one or more additional outbreaks. Authorities of the early 1890s recognized that the diagnosis of influenza was difficult, and that mild cases were easily confused with other respiratory and catarrh-like disorders. They were quite certain from clinical and epidemiological records that the influenza of the great pandemic of 1889–1890 was the same disease that had caused the influenza pandemics of the past, such as that of 1848–1849. The more vexing problem was whether this pandemic influenza was the same disease as the disorder commonly known as influenza or grippe that occurred almost every year. Parsons thought they undoubtedly were distinct diseases; Leichtenstern agreed, although less adamantly.
1,
3 (p. 81) (p. 530–1)
Go to:
INFLUENZA TYPES
Its clinical features and its opaque identity made influenza seem an especially protean disease. Writing in 1907, Clifford Allbutt, Regius Professor of Medicine, “observed influenza is of protean diseases the most protean; more diversified even than syphilis.”
7 (p. 1) Individual cases were characterized by their sudden onset and by extreme prostration, which was out of all proportion to other pathological features. The disease's regular target was the respiratory tract, and pneumonia was the most serious complication of influenza and the major cause of mortality during an outbreak. But Leichtenstern observed that cases might exhibit no respiratory symptoms at all. In addition to the typical respiratory cases, both he and Parsons passed on a division of three subtypes inherited from earlier authors: nervous, catarrhal, and gastric.
1,
3 (p. 64) (p. 590–1) In succeeding years, the number of recognized clinical types swelled enormously. In 1907, when Frederick Lord wrote his chapter on influenza in Osler's multi-volume reference work,
Modern Medicine, he described no fewer than 10 clinical types, including influenza of the circulatory system, of the genito-urinary system, of the joints, and of the skin.
6 (p. 474–83) Influenza, it seems, was having an identity crisis. This is a point to which we will return.
The generation working after the pandemic of 1889–1890 also classified influenza cases according to their occurrence and presumed cause. Leichtenstern proposed a tripartite division of influenza types: pandemic
influenza vera (the disease that occurred in great global outbreaks), endemic-epidemic
influenza vera (the disease having the same cause but which occurred in smaller outbreaks following a pandemic), and endemic
influenza nostras (pseudo-influenza due to different causes).
3 (p. 531) Both Osler and Lord passed on this classification to their readers, although Lord significantly altered the third category to endemic
influenza vera, suggesting that cases in this classification must have the same cause as those occurring in epidemics
5,
6 (p. 116) (p. 473).
The experience with the 1889–1890 pandemic taught medical authorities that pandemic influenza was a disease of very high morbidity and low case fatality, although it seemed that in the outbreaks immediately following a pandemic, morbidity rates could be expected to decline and case fatality rates to rise. Given the problems of differential diagnosis and the existence of mild cases, exact statistics were difficult to obtain. Authorities concluded, however, that in 1889–1890 the infection was very widely distributed in European nations. Leichtenstern estimated that as much as 50% of the German population had been infected, while Parsons put the estimate for Greater London at 25%. Reported incidence rates for employees of British institutions ranged from 9% for troops stationed in Britain to 33% for postal employees.
1,
3 (p. 3–7, 109–10) (p. 532, 564–70)
The experience of 1889–1890 suggested that pandemic influenza had distinct patterns of age-specific morbidity and mortality. Continental figures indicated that morbidity was highest between ages 20 and 40 and lowest after age 50, while case fatality rates were highest among the elderly. Deaths registered as due to influenza in England and Wales were highest in the age group 40–60 at 36%, while 24% of influenza deaths took place between the ages of 20 and 40 and 22% between the ages of 60 and 80. Parsons demonstrated that this mortality pattern was very different from that of the inter-pandemic period. Between 1876 and 1889, 33% of deaths attributed to influenza occurred in the first year of life and another 34% occurred after age 60.
1 (p. 6)
Go to:
THE BACTERIOLOGY OF INFLUENZA
During the pandemic of 1889–1890, researchers used the new methods of medical microbiology in unsuccessful efforts to identify the microbial cause of influenza. An apparent breakthrough came in 1892, during a subsequent outbreak, when Richard Pfeiffer announced in a single-page preliminary publication,
8 and a year later in a more substantial article, that he had found influenza's cause.
9 Pfeiffer reported finding in every case of influenza he examined a rod-shaped organism. In uncomplicated cases he found these bacilli in overwhelming numbers and frequently in pure culture. Pfeiffer's bacillus was challenging to work with. It was very small and fastidious. It would only grow on blood argar plates. It could not be stained with Gram's stain, but it would accept Loeffler's methylene blue stain, and it displayed characteristic polar staining, making it easy to confuse with diplococci. Pfeiffer was never able to find an animal model for influenza, although he innoculated mice, rats, guinea pigs, rabbits, pigs, cats, dogs, and monkeys. To further complicate matters, although he had focused his investigation almost exclusively on influenza cases, he reported finding in a few cases of “diphtheric bronchopneumonia” a bacillus that was indistinguishable from his own bacillus on the grounds of morphology and of culture and staining characteristics. He labeled this organism pseudo-influenza bacillus.
In retrospect, Pfeiffer's chain of evidence may seem more shaky than it did to his contemporaries. Pfeiffer, a protege of Robert Koch, was, after all, a productive and distinguished bacteriologist. Contemporaries respected the technical skill he exhibited in isolating and characterizing his bacillus. The failure to satisfy Koch's Postulates by producing an experimental disease in animals by the inoculation of pure culture was not in itself damning. Koch, himself, had sometimes failed in this regard. The existence of the pseudo-influenza bacillus would seem to his contemporaries no more implausible than the existence of the pseudo-diphtheria bacillus. While the scientific response to Pfeiffer's discovery is difficult to characterize concisely, it does seem fair to conclude that most medical authorities believed that Pfeiffer was basically correct in his identification, even though his evidence might not be complete. (Although the organism that Pfeiffer isolated was most likely what we know today as
Hemophilus influenzae, we refer to it in this article in the way it was referred to during the period under discussion: Pfeiffer's bacillus and
Bacillus influenzae [
B. influenzae]).
Parsons published before Pfeiffer's announcement, but Leichtenstern published three years after, and he endorsed Pfeiffer's discovery with only modest qualification. “Should the
Bacillus influenzae, discovered by R. Pfeiffer in 1892, continue to maintain in future pandemics its place as the exclusive cause of the disease, as may certainly be expected, its discovery may be considered as the most important achievement of our latest influenza pandemic.”
3 (p. 524)
In succeeding years there was keen interest in Pfeiffer's bacillus. In 1892, when Pfeiffer announced the discovery of
B. influenzae, Americans had little, if anything, to add to the discussion. By 1918, on the other hand, they were active participants. By that time, laboratory courses in medical bacteriology were being taught in most American medical schools, diagnostic laboratories operated in many hospitals and in some public health departments, and in some laboratories American bacteriologists were already doing world-class research. The active participation of medical officers in the U.S. Army in 1918 and 1919 is an indication of how widely disseminated the new laboratory techniques were in the American medical profession. These laboratories may seem rudimentary by 21st century standards. Microorganisms were identified primarily by morphology and by basic culture and staining techniques. Routine clinical diagnosis, sputum examinations for tuberculosis, and throat cultures for diphtheria, for example, had begun to exploit these basic laboratory techniques. More specialized techniques, such as the Widal examination of typhoid fever and complement fixation tests such as the Wassermann test for syphilis, were early examples of the exploitation of immunological phenomena. Filterable viruses were known to exist, but very little was known about them, and there were very few techniques for working with them.
In the years immediately following Pfeiffer's discovery, many investigators confirmed his findings by isolating his bacillus from influenza cases. But there were complications. Others reported isolating organisms indistinguishable by contemporary laboratory methods from
B. influenzae from other diseases and even from normal throats.
10 (p. 28–32) For example David J. Davis, from the Memorial Institute for Infectious Diseases in Chicago, reported in 1906 isolating Pfeiffer's bacilli from all but five of the series of 61 cases of whooping cough he studied. He also found them in 40% to 80% of a smaller number of cases of cerebro-spinal meningitis, varicella, measles, and bronchitis. Significantly, he succeeded in isolating Pfeiffer's bacilli in only three (18%) of 17 cases of influenza.
10 (p. 12–3, 25–8)
Such results suggested to some that Pfeiffer's bacillus was merely a secondary invader. But these findings might also indicate that this organism was a key player in a more complex etiology. W. D'Este Emery, clinical pathologist at King's College Hospital, London, drew attention to the fact that
B. influenzae grew more readily in culture in the presence of other organisms and seemed to be more virulent for animals in the presence of killed streptococci. Emery wondered whether Pfeiffer's bacillus might be a “harmless saprophyte” most of the time but be capable in the presence of other pathogens of being transformed into “the pathogenic bacillus which occurred in the pandemic of the nineties.”
11 (p. 110)
The confusion over the etiology of influenza on the eve of the pandemic of 1918–1919 is well illustrated in the eighth edition of Osler's textbook of 1912. In the definition of the disease he states that “a special organism,
Bacillus influenzae, is found,” and in the section on bacteriology he also states that this organism “is recognized as the cause of the disease,” but he also points out that it is commonly found in other diseases and is “probably constantly with us.”
5 (p. 115–7) Despite such reservations, medical authorities recognized that Pfeiffer's bacillus was the only viable candidate for the cause of influenza. On the eve of the pandemic of 1918–1919, it was deeply implicated in the understanding and even the definition of the disease. That great expansion in clinical types of influenza identified in Frederick Lord's synthesis of scientific knowledge was made possible because
B. influenzae had been isolated from the blood, from heart valves, from the joints, and from the urinary tract. In an age when etiological definitions of disease were of growing importance and bacteriology was beginning to provide the gold standard for differential diagnosis in infectious diseases, Pfeiffer's bacillus had become indispensable.
Go to:
INFLUENZA VACCINES
The fate of Pfeiffer's bacillus as the probable cause of influenza is reflected in the use of vaccines in the United States during the pandemic of 1918–1919. By 1918, the successful use of some vaccines, especially those against rabies, typhoid fever, and diphtheria, as well as the use of diphtheria anti-toxin, had raised high expectations for a vaccine against influenza.
12 Those who already had a vaccine in hand were quick off the mark to promote their vaccines as sure preventives or cures for influenza. Drug manufacturers aggressively promoted their stock vaccines for colds, grippe, and flu. These vaccines were of undisclosed composition. As public anxiety and demand swelled, there were complaints of price gouging and kickbacks.
13 (p. 114–6) Preexisting vaccines of undisclosed composition were also endorsed by physicians such as M.J. Exner, who actively promoted in newspaper interviews and testimonials the vaccine developed some six years earlier by his colleague, Ellis Bonime.
14,
15 Bonime was a late champion of the tuberculin treatment of tuberculosis and an adherent of the opsonin theory of immune response and of the therapeutic use of vaccines.
16 His vaccine was claimed to prevent pneumonia, influenza, and blood poisoning. Exner's boosterism paid some dividends. At least one municipality, Far Rockaway, New York, announced that it would provide Bonime's vaccine to all its citizens.
17
Early in the pandemic, more highly respected and well-placed authorities developed vaccines based explicitly on Pfeiffer's bacillus. On October 2, 1918, Royal S. Copeland, Health Commissioner of New York City, sought to reassure citizens that help was on the way, because the director of the Health Department's laboratories, William H. Park, was developing a vaccine that would offer protection against this dreaded disease.
18 Park's successes in combating diphtheria with anti-toxins and vaccines developed in these same laboratories gave Copeland's announcement much weight. Park explained to his colleagues that he and his staff consistently had been able to isolate Pfeiffer's bacillus from influenza cases, and that his laboratory had isolated the current strain, shown that animals injected with it developed specific antibodies, and developed a heat-killed vaccine that was to be administered in three doses at two-day intervals.
19
Park's was not the only Pfeiffer's bacillus influenza vaccine to make an early appearance during the pandemic. At Tufts Medical School in Boston, Timothy Leary, professor of bacteriology and pathology, developed another Pfeiffer's bacillus vaccine. His was developed from three locally isolated strains, and it was heat-killed and chemically treated. Leary promoted his vaccine as both a preventive and a treatment for influenza.
20 Other Pfeiffer's bacillus vaccines soon followed. Faculty from the Medical School of the University of Pittsburgh isolated 13 strains of the Pfeiffer's bacillus and produced a vaccine from them by modifying the techniques Park had used. In the crisis atmosphere of the pandemic, the Pittsburgh vaccine developers isolated their strains, prepared the vaccine, tested it for toxicity in some laboratory animals and in two humans, and turned it over to the Red Cross for use in humans—all in one week.
13 (p. 109–11) In New Orleans, Charles W. Duval and William H. Harris from Tulane University's Department of Pathology and Bacteriology developed their own chemically killed Pfeiffer's bacillus vaccine. Their justification for its use was the common presence of the bacillus in influenza cases and the example of the typhoid vaccine whose administration schedule they followed.
21
It was not only heads of bacteriological laboratories who acted on the assumption that Pfeiffer's bacillus was the cause of influenza and developed vaccines on that assumption. Some private physicians did the same. Horace Greeley of Brooklyn, New York, reported isolating 17 strains of the bacillus from 17 patients, and from these “strains,” he developed a heat-killed vaccine intended to be administered in three increasing doses. With it he immunized his own patients, and he distributed eight liters to colleagues who did the same.
22
These vaccines were widely used. Park's vaccine was released to the military for use in Army camps as well as to private physicians. It was also used as corporate policy among industrial workers, including the 14,000 employees of the Consolidated Gas Company and 275,000 employees of the U.S. Steel Company.
17,
19,
23 Leary's vaccine was used frequently during the epidemic in state custodial institutions of the Northeast and by some private physicians.
13 (p. 105–7),
24–
27 Duval and Harris reported immunizing approximately 5,000 people, most of whom were employees of large New Orleans companies.
21 (p. 320–2) Almost without exception, those reporting on the use of these Pfeiffer's bacillus vaccines reported that they were effective in preventing influenza.
Go to:
THE FALTERING CASE FOR PFEIFFER'S BACILLUS
At first the apparent success of these vaccines served to increase confidence in the role played by Pfeiffer's bacillus. But other evidence was accumulating. Initially, when observers reported difficulty isolating Pfeiffer's bacillus from influenza cases, they found their technique and experience questioned.
28,
29 (p. 320) But slowly the evidence against Pfeiffer's bacillus mounted, first ambiguously and then emphatically. J.J. Keegan, a naval medical officer working in the Boston area, published an early report on studies undertaken during an outbreak of 2,000 cases in the First Naval District during the two-week period between August 28 and September 11, 1918. Keegan made a special effort to study the outbreak bacteriologically. He had difficulty isolating Pfeiffer's bacillus from throat washings or from sputum in both influenza cases and from patients admitted to the hospital with other conditions. He wondered whether the organism might be harbored in the sinuses or some other place more inaccessible to him. When he resorted to lung punctures in life and lung cultures at postmortem, he succeeded in isolating Pfeiffer's bacillus in 82.6% of 23 cases.
30 (p. 1053–5)
Other ambiguous results came from Edwin Jordan, a future American influenza expert. Jordan reported on a large bacteriological study of patients diagnosed with influenza and with other diseases during and after the epidemic at the University of Chicago. He reported finding no consistent bacteriology in his cases. No microorganism was present in all influenza cases. Although he identified Pfeiffer's bacillus in 64% of influenza cases, and this was more frequent than any other organism, its relative abundance varied a great deal among cases. He also isolated
B. influenzae in 14% of colds and other infections.
31,
32
A group from the medical staff of Cook County Hospital in Chicago undertook a careful study using 3,000 blood agar culture plates and procedures that they held should have detected
B. influenzae, if it were present. They found that Pfeiffer's bacillus was present in only a small number of cases: in only 4% of cultures made from washed sputum samples and in only 8.7% of postmortem lung cultures. They did find the organism in near pure culture in the lungs of a soldier who had died of influenzal pneumonia. They regarded Pfeiffer's bacillus as the cause of that case of pneumonia. They found that pneumococci were the most common organisms isolated in this study, appearing in 70% of sputum cultures and in 38% of throat swab cultures. Type IV pneumococci were isolated in 50% of lung cultures made at autopsy. Types I–III were all also present but at lesser frequencies.
33
By early 1919, evidence was running more strongly against Pfeiffer's bacillus. In February, David Davis, employing strict morphological and culture criteria, reported that he had succeeded in isolating what he identified as
B. influenzae in only 8% of 62 cases of influenza he studied. As noted, he had earlier isolated this organism in higher percentages of cases of measles, varicella, tuberculosis, and pertussis. There was no doubt, he argued, that Pfeiffer's bacillus was pathogenic for humans. He had isolated it from the spinal fluid in all cases of meningitis accompanying bronchopneumonia where
B. influenzae was also present in pure or nearly pure culture. He concluded that whatever the cause of influenza might be, its most serious features were due to secondary invaders including streptococci, pneumococci, and
B. influenzae.
34 Frederick Lord and colleagues at Boston reached similar conclusions. Like Davis, Lord had already isolated
B. influenzae from diseases other than influenza. In this pandemic, he and his colleagues isolated organisms resembling Pfeiffer's bacillus in 84% of 38 hospitalized influenza cases, but also in 41% of the throats of members of the Harvard Students' Army Training Corps, who had no record of illness for the previous three months. Lord concluded that
B. influenzae should be regarded as a part of the normal flora of the human throat, but that there was no way to be certain whether the organisms found in normal throats and in other diseases with similar morphology and culture and staining characteristics were really identical to those found in influenza.
35
There remained, it seemed, a possibility that would clarify recent bacteriological findings and still rescue a place for Pfeiffer's bacillus in the etiology of influenza. Perhaps, as would prove to be the case with diphtheria, there was a pseudo-influenza bacillus or different strains of
B. influenzae, not all of which caused influenza. In that case, the finding of organisms morphologically identical to Pfeiffer's bacillus in other diseases was not evidence against the role of Pfeiffer's bacillus in influenza.
Several researchers investigated this possibility by trying to type strains of Pfeiffer's bacillus, but their findings did little to buttress faith in
B. influenzae's role in influenza. F.H. Rapoport, a naval medical officer from Chelsea, Massachusetts, employed the complement fixation test for antibodies to
B. influenzae in convalescent sera from cases of influenzal pneumonia and from normal control sera. He concluded that specific antibodies against Pfeiffer's bacillus were formed during convalescence from pneumonia accompanying influenza, but that these had weak complement-binding properties. He could not determine whether one or more strains of Pfeiffer's bacillus were circulating during the epidemic, although he observed that polyvalent antigens in his samples gave no better results than did monovalent ones.
36
Park and his associates studied cultures taken from 100 cases of influenza. In some cases, cultures were taken repeatedly over time. Careful antigen typing showed that there was a large variety of types of
B. influenzae, that the organisms taken from an individual were quite stable over time, but that there were differences among the many types isolated from different individuals. He suggested that, like pneumococcus,
B. influenzae had over the years in the throats of healthy carriers altered into distinct types. Pfeiffer's bacillus in cases of influenza, he concluded, must be regarded as a secondary invader.
29 (p. 320–1)
Go to:
ALTERNATIVE ETIOLOGIES, OTHER VACCINES
Other candidates had been proposed as the cause of influenza during the pandemic, but these were disposed of rather quickly. An Army medical officer, Captain George Mathers, who died of influenza during his investigation, isolated and characterized a streptococcus that produced a green color on blood agar plates. At Fort Mead, he isolated his green-producing streptococcus from 87% of influenza and pneumonia cases, while he was able to isolate Pfeiffer's bacillus in only 58% of these cases.
37
The Mathers streptococcus attracted some attention during the early months of the pandemic. Jordan, for example, systematically looked for it in his study but found no evidence that made it seem a more probable cause than
B. influenzae. Then, in both Europe and America, investigators considered the possibility that influenza might be caused by a filterable virus.
34 (p. 148–9) At issue was the disputed finding that influenza could be caused in humans by inoculation of material from the noses or throats of influenza patients that had been passed through a bacterial filter. French and Japanese investigators had reported succeeding in transferring influenza by this method.
38,
39 American researchers failed to confirm these findings. The researchers from Cook County Hospital used this method to inoculate seven human volunteers without causing disease. They did the same with cultures made from the lungs of influenza pneumonia victims and inoculated two Rhesus monkeys with similar results.
33 (p. 1564–5) Other laboratory and human inoculation experiments aimed at detecting a filterable virus were also negative.
40,
41 These negative findings were also confirmed by extensive human experiments with influenza sponsored by the U.S. Navy and the U.S. Public Health Service.
As confidence in the role of Pfeiffer's bacillus in influenza waned, the strategy of prevention by vaccine changed. Vaccines developed later in the pandemic—and almost all developed in the middle of the country and on the West Coast—were composed of other organisms either singly or in mixtures. Increasingly, vaccines were justified as preventing the pneumonias that accompanied influenza. Killed streptococci vaccines were developed by a physician in Denver and by the medical staff of the Puget Sound Naval Yard.
42,
43 The latter was used among sailors and also among civilians in Seattle.
Mixed vaccines were more common. These typically contained pneumococci and streptococci. Sometimes staphylococci, Pfeiffer's bacillus, and even unidentified organisms recently isolated in the ward or morgue were included.
44–
47 The most widely used, and historically the most interesting, was the vaccine produced by Edward C. Rosenow of the Mayo Clinic's Division of Experimental Bacteriology.
48,
49 Rosenow argued that the exact composition of a vaccine intended to prevent pneumonia had to match the distribution of the lung-infecting microbes then in circulation. For that reason, he insisted that the composition of his vaccine had to be frequently readjusted. His initial vaccine consisted of killed bacteria in these proportions: 30% pneumococci types I, II, and III; 30% pneumococci type IV and a “green-producing diplostreptococcus;” 20% hemolytic streptococci; 10% staphylococcus aureus; and 10%
B. influenzae. He later dropped Pfeiffer's bacillus entirely. The Mayo Clinic distributed Rosenow's vaccine widely to physicians in the upper Midwest. No one seems to know for sure how many people received this vaccine, but, through physicians, Rosenow received returns for 93,000 people who had received all three injections, 23,000 who had received two injections, and 27,000 who had received one.
49 (p. 398) Rosenow's vaccine received even wider distribution. It was adopted by the City of Chicago. The Laboratories of the Chicago Health Department produced more than 500,000 doses of the vaccine. Some of it was distributed to Chicago physicians and the rest was turned over to the state health department for use throughout Illinois.
50 (p. 116–23)
51,
52
Go to:
VACCINE CONTROVERSY AND STANDARDS FOR VACCINE TRIALS
As was the case with Pfeiffer's bacillus vaccines, most of the early reports on the use of these mixed vaccines indicated they were effective. Readers of American medical journals in 1918 and for much of 1919 were thus faced with the strange circumstance that all vaccines, regardless of their composition, their mode of administration, or the circumstances in which they were tested, were held to prevent influenza or influenzal pneumonia. Something was clearly wrong. The medical profession had at the time no consensus on what constituted a valid vaccine trial, and it could not determine whether these vaccines did any good at all. The lack of agreed-upon standards was exacerbated by the informal editorial procedures and the absence of peer review in scientific publication in 1918. During the pandemic of 1918–1919, the profession was forced to develop standards for vaccine trials.
53 Park and George McCoy, director of the Hygienic Laboratory of the Public Health Service, led the assault pointing out the fallacies in design or inference of current reports. Most trials began after the first cases of influenza had appeared locally, often after the epidemic peak had passed, and hence the most susceptible may already have been attacked and could not appear in the vaccinated group, and the more resistant were likely to be assigned to the vaccinated group. Little effort was usually made to minimize selection bias in assignments to experimental or control arms or to match each group by age, sex, and exposure. And too many trials operated with poor observation and imperfect data collection.
54,
55 (p. 103)
McCoy arranged his own trial of the Rosenow vaccine produced by the Laboratories of the Chicago Health Department. He and his associates worked in a mental asylum in California where they could keep all subjects under close observation. They immunized alternate patients younger than age 41 on every ward, completing the last immunization 11 days before the local outbreak began. Under these more controlled conditions, Rosenow's vaccine offered no protection whatsoever. McCoy's article appeared as a one-column report in the December 14, 1918, edition of the
Journal of the American Medical Association (
JAMA).
56
At the meeting of the American Public Health Association (APHA) later that month, McCoy and Park used their positions on the Executive Sub-committee on the Bacteriology of the 1918 Epidemic of Influenza to issue a manifesto that appeared in APHA's “Working Program against Influenza.”
57 APHA declared that because the cause of influenza was unknown, there was no logical basis for a vaccine to prevent the disease. There was a logical basis for believing that a vaccine to prevent the secondary infections might be developed, but there was no evidence that any of the vaccines currently available were effective. The association then specified the criteria that a trial must meet, if its conclusions were to be valid. There must be a control group, the association specified, and the vaccinated and the control group must be equal in size. The relative susceptibilities of the two groups must be equivalent as determined by age, sex, and prior exposure. Their degree of exposure must be of equal duration and intensity, and should take place during the same phase of the epidemic.
57 (p. 3)
The reformers' campaign had an impact. Following its publication—although the basic design faults of many trials remained—some authors now acknowledged shortcomings in their data or qualified their conclusions, and a few cited APHA's new standards as authoritative.
53 (p. 418–9) By the beginning of 1919, Rosenow, the most vocal defender of vaccines, found himself on the defensive. During the discussion of his paper at APHA's annual meeting, he faced hostile comments from both McCoy and Victor Vaughan.
58 (p. 2098–100) The next month,
JAMA ran an anonymous critical editorial accompanying his first article on the use of his vaccine.
59 Perhaps the best evidence that professional standards were changing is found in two studies sponsored by the Metropolitan Life Insurance Company during the 1919–1920 influenza season. Both were unprecedented in the influenza literature in the care taken in trial design and analysis. Park and his associate, Anna Von Sholly, studied the use of two mixed vaccines among the employees of the home office of Met Life.
55 Edwin Jordan and W.B. Sharp studied the effects of a single mixed vaccine in three residential schools and two large mental hospitals in Illinois.
60 While adhering to the standards APHA had set forth, both studies concluded the vaccines used were ineffective.
Go to:
EPIDEMIOLOGICAL STUDIES
American epidemiologists also devoted much attention to the 1918–1919 pandemic. Some of their studies—such as the substantial study on the epidemic in Connecticut by Winslow and Rogers,
61 or the study of trends from 1910 to 1918 that W.H. Frost prepared for the Public Health Service,
62 or Raymond Pearl's statistical analysis of the epidemic curves of major American cities
63—were large-scale studies based on mass mortality data. Some of the more illuminating, however, were smaller-scale studies in which chains of transmission could be traced and incubation periods estimated in small, isolated populations such as inmates in a prison
64 or residents on a small island.
65 Among the most important were studies that acknowledged that accurate information on cases of influenza, rather than simply influenza and pneumonia deaths, was both lacking and critically important. The Public Health Service made a major effort to obtain records of illness through household surveys it conducted in 10 communities across the nation in which it was already doing research.
66,
67 A more intensive study was undertaken by Warren T. Vaughan in a population of 10,000 in six carefully chosen districts in Boston during the 1920 flu season.
68 He also obtained information retrospectively on household illness during 1918–1919.
This epidemiological research confirmed many of the findings from 1889–1890 about pandemic influenza's rapid spread, explosive local outbreaks, and very high morbidity rates. Frost's analysis of the household returns show a range of local influenza morbidity rates ran from 150 to 530 cases per 1,000, although both he and Vaughan concluded that 200 per 1,000 was more typical for 1918–1919.
66,
68 (p. 588) (p. 142) Those enormously high rates of incidence explained how a disease with case fatality rates these authors found to range from 0.8% to 3.1% could cause so many deaths.
66,
68 (p. 593) (p. 165) These studies also showed that differences in case fatality rates were more important than differences in incidence rates in explaining the age group mortality patterns, including the high death rates among young adults during the pandemic.
66 (p. 588–96)
Vaughan was unusual in paying attention to the question of population immunity. Although the cause of influenza must have been widely distributed in his districts in 1918–1919, some people showed remarkable resistance to the disease. Fifty-five percent of those in his study groups who shared a bed with an influenza victim during the pandemic escaped the disease. He argued that the patterns of incidence and death during the 1918–1919 pandemic could not be explained by immunity acquired during the pandemic of 1889–1890, and he suggested, perhaps more sagaciously than he realized, that understanding of herd immunity would be the key to understanding the epidemiology of influenza. If measles produced no lasting immunity, he pointed out, its outbreaks in cities would be as explosive as those of the great pandemic of 1918–1919.
68 (p. 209–10, 230–2)
Perhaps the most interesting epidemiological studies conducted during the 1918–1919 pandemic were the human experiments conducted by the Public Health Service and the U.S. Navy under the supervision of Milton Rosenau on Gallops Island, the quarantine station in Boston Harbor, and on Angel Island, its counterpart in San Francisco. The experiment began with 100 volunteers from the Navy who had no history of influenza. Rosenau was the first to report on the experiments conducted at Gallops Island in November and December 1918.
69 His first volunteers received first one strain and then several strains of Pfeiffer's bacillus by spray and swab into their noses and throats and then into their eyes. When that procedure failed to produce disease, others were inoculated with mixtures of other organisms isolated from the throats and noses of influenza patients. Next, some volunteers received injections of blood from influenza patients. Finally, 13 of the volunteers were taken into an influenza ward and exposed to 10 influenza patients each. Each volunteer was to shake hands with each patient, to talk with him at close range, and to permit him to cough directly into his face. None of the volunteers in these experiments developed influenza. Rosenau was clearly puzzled, and he cautioned against drawing conclusions from negative results. He ended his article in
JAMA with a telling acknowledgement: “We entered the outbreak with a notion that we knew the cause of the disease, and were quite sure we knew how it was transmitted from person to person. Perhaps, if we have learned anything, it is that we are not quite sure what we know about the disease.”
69 (p. 313)
The research conducted at Angel Island and that continued in early 1919 in Boston broadened this research by inoculating with the Mathers streptococcus and by including a search for filter-passing agents, but it produced similar negative results.
70–
72 It seemed that what was acknowledged to be one of the most contagious of communicable diseases could not be transferred under experimental conditions.
Go to:
THE PANDEMIC AND BIOMEDICAL KNOWLEDGE
While the experience of the great pandemic of 1918–1919 had given American medical researchers a heightened appreciation of the dangers of pandemic influenza, and while it permitted epidemiologists to enlarge the fund of descriptive information on influenza outbreaks, it had done little to unlock the mysteries of the disease. If anything, the experience of 1918–1919 served to deconstruct existing biomedical knowledge.
This void in fundamental knowledge would not be filled soon. When Jordan published his massive, 500-page authoritative synthesis of the influenza literature in 1927, the most basic and fundamental features of influenza were still unexplained. Jordan told his readers that influenza could only be defined by its pattern of occurrence—its epidemiology. Its cause was unknown, and its pathology was indefinite. It was uncertain whether there was acquired immunity for influenza, and, if there was, how long it lasted. Why pandemics occurred when they did and why they spared some places were also unknown. It was also uncertain whether the disease called influenza that occurred every year in sporadic cases and small outbreaks was the same disease that circulated in the pandemics. He continued the practice of distinguishing “influenza” from “epidemic influenza.”
73
Jordan did suggest that changes in virulence of the still unknown agent of influenza might be important and that this agent might be filterable, but in 1927 these were still speculations for which there was no direct evidence. In short, the three decades that had passed since Leichtenstern published his major synthesis had seen remarkably little addition to the fund of basic scientific knowledge of influenza, in spite of concerted efforts by researchers employing the best available research tools.
Go to:
REFERENCES
1. Parsons F. Report on the influenza epidemic of 1889–90 [C.—6387] London: HMSO; 1891. p. 324. [
Google Scholar]
2. Leichtenstern OML. Influenza and dengue. In: Northnagel H, editor. Vienna: A. Hölder; 1896. p. 222. Specielle Pathologie und Therapie; Band 4. [
Google Scholar]
3. Leichtenstern OML. Influenza. In: Mannaberg J, Leichtenstern OML, Ross R, Stephens JWW, Grunbaum AS, editors; Stengel A, translator. Malaria, influenza, and dengue. Philadelphia/London: W.B. Saunders; 1905. pp. 523–719. [
Google Scholar]
4. Osler W. Principles and practice of medicine. 2nd ed. New York: D. Appleton; 1895. Influenza; pp. 92–4. [
Google Scholar]
5. Osler W. Principles and practice of medicine. 8th ed. New York: D. Appleton; 1912. Influenza; pp. 115–9. [
Google Scholar]
6. Lord FT. Influenza. In: Osler W, McCrae T, editors. Modern medicine: its theory and practice. Vol. 2. Philadelphia/New York: Lea Brothers; 1907. pp. 469–88. [
Google Scholar]
7. Allbutt TC. Influenza: introduction. Practitioner. 1907;78:1–10. [
Google Scholar]
8. Pfeiffer R. Vorlaufige Mittheilungen uber die Erreger der Influenza. Deutsche med. Wchschr. 1892;18:28. [
Google Scholar]
9. Pfeiffer R. Die Aeteiologie der Influenza. Ztschr. f. Hyg. u. Infektionskr. 1893;13:357–86. [
Google Scholar]
10. Davis DJ. The bacteriology of whooping cough. J Infect Dis. 1906;3:1–37. [
Google Scholar]
11. Emery WD'E. The micro-organisms of influenza. Practitioner. 1907;78:109–17. [
Google Scholar]
12. Hansen B. New images of a new medicine: visual evidence for the widespread popularity of therapeutic discoveries in America after 1885. Bull Hist Med. 1999;73:629–78. [
PubMed] [
Google Scholar]
13. Haythorn SR. Studies on epidemic influenza comprising clinical and laboratory investigations by members of the faculty of the School of Medicine, University of Pittsburgh. Pittsburgh: University of Pittsburgh Medical School; 1919. The prevention of epidemic influenza with special reference to vaccine prophylaxis; pp. 97–153. [
Google Scholar]
14. 903 new cases of grip reported yesterday—use of vaccine not new. New York Times. 1918 Oct 3;:24. [
Google Scholar]
15. Grip in the Y.M.C.A checked by vaccine. New York Times. 1918 Oct 17;:9. [
Google Scholar]
16. Bonime E. Tuberculin and vaccine in tubercular affections: a practical guide for the utilization of the immune response in general practice. Troy (NY): Southworth; 1917. p. 267. [
Google Scholar]
17. Copeland sees grip on the wane here. New York Times. 1918 Oct 25;:22. [
Google Scholar]
18. Tells of vaccine to stop influenza. New York Times. 1918 Oct 2;:10. [
Google Scholar]
19. Park WH. Bacteriology and possibility of antiInfluenza vaccine as a prophylactic. N Y Med J. 1918;108:621. [
Google Scholar]
20. Leary T. The use of influenza vaccine in the present epidemic. Am J Public Health. 1918;8:754–5. 768. [
PMC free article] [
PubMed] [
Google Scholar]
21. Duval CW, Harris WH. The antigenic property of the Pfeiffer bacillus as related to its value in the prophylaxis of epidemic influenza. J Immunology. 1919;4:317–30. [
Google Scholar]
22. Greeley H. Vaccine as a prophylactic against influenza, and local reaction as a guide to immunity. Med Rec. 1919;96:624–7. [
Google Scholar]
23. Big firms take up fight on influenza. New York Times. 1918 Oct 23;:8. [
Google Scholar]
24. Hinton WA, Kane ES. Use of influenza vaccine as a prophylactic—an experimental study conducted by the Massachusetts State Department of Health. J Tennessee State Med Assn. 1918;11:442–6. [
Google Scholar]
25. Barnes HL. The prophylactic value of Leary's vaccine. JAMA. 1918;71:1899. [
Google Scholar]
26. Hawes JB. Experience of Massachusetts State sanatoria for tuberculosis during the recent influenza epidemic. Boston Med Surg J. 1919;180:35–7. [
Google Scholar]
27. Wallace GL. Report of the influenza epidemic and experience in the use of the influenza vaccine `B' at the Wrentham State School, Wrentham, Mass. Boston Med Surg J. 1919;180:447–48. [
Google Scholar]
28. The factor of technique in the detection of the influenza bacillus. Public Health Rep. 1919;34:1973. [
Google Scholar]
29. Park WH. Bacteriology of recent pandemic of influenza and complicating infections. JAMA. 1919;73:318–21. [
Google Scholar]
30. Keegan JJ. The prevailing pandemic of influenza. JAMA. 1918;71:1051–5. [
Google Scholar]
31. Jordan EO. Observations on the bacteriology of influenza. Public Health Rep. 1919;34:1413–25. [
Google Scholar]
32. Jordan EO. Observations on the bacteriology of influenza. J Infect Dis. 1919;25:28–40. [
Google Scholar]
33. Nuzum JW, Pilot I, Stangl FH, Bonar BE. Pandemic influenza and pneumonia in a large civil hospital. JAMA. 1918;71:1562–5. [
PubMed] [
Google Scholar]
34. Davis DJ. The bacteriology of influenza. Proc Inst Med Path. 1919;2:142–50. [
Google Scholar]
35. Lord FT, Scott AC, Jr, Nye RN. Relation of influenza bacillus to the recent epidemic of influenza. JAMA. 1919;72:188–90. [
Google Scholar]
36. Rapoport FH. The complement fixation test in influenzal pneumonia: studies with serum from convalescent patients, the influenza bacillus being used as antigen. JAMA. 1919;72:633–6. [
Google Scholar]
37. Tunnicliff R. Phagocytic experiments in influenza. JAMA. 1918;71:1733–4. [
Google Scholar]
38. Nicolle C, Lebailly C. Recherches experimentales sur la grippe. Ann De l'Inst Pasteur. 1919;33:395–402. [
Google Scholar]
39. Yamanouchi T, Sakakami K, Iwashima S. The infecting agent in influenza: an experimental research. Lancet. 1919;1:971. [
Google Scholar]
40. Branham SE, Hall IC. Attempts to cultivate filterable viruses from cases of influenza and common colds. J Infect Dis. 1921;28:143–9. [
Google Scholar]
41. Wahl HR, White GB, Lyall HW. Some experiments on the transmission of influenza. J Infect Dis. 1919;25:419–26. [
Google Scholar]
42. Katzman M. Influenza vaccination at the Denver City and County Hospital. Colorado Med. 1919;16:121–3. [
Google Scholar]
43. Ely CF, Lloyd BJ, Hitchcock CD, Nickson DH. Influenza as seen at the Puget Sound Navy Yard. JAMA. 1919;72:24–8. [
Google Scholar]
44. Minaker AJ, Irvine RS. Prophylactic use of mixed vaccine against pandemic influenza and its complications at the Naval Training Station, San Francisco. JAMA. 1919;72:847–50. [
Google Scholar]
45. Watters WH. Vaccines in influenza. Boston Med Surg J. 1919;181:727–31. [
Google Scholar]
46. Stone WB. A prophylactic vaccine against the so-called Spanish influenza. Med Rec. 1918;94:979–80. [
Google Scholar]
47. Kolmer JH. The value of active immunization with vaccine virus against influenza. Med Rec. 1918;94:919. [
Google Scholar]
48. Rosenow EC. Prophylactic inoculation against respiratory infections during the present pandemic of influenza. Preliminary report. JAMA. 1919;72:31–4. [
Google Scholar]
49. Rosenow EC, Sturdivant BF. Studies in influenza and pneumonia. IV. Further results of prophylactic inoculations. JAMA. 1919;73:396–401. [
Google Scholar]
50. Report and handbook of the Department of Health of the City of Chicago, 1911–1918 inclusive. Chicago: Chicago Department of Health; 1919. Report of an epidemic of influenza in Chicago during the fall of 1918; pp. 40–150. [
Google Scholar]
51. Illinois Influenza Commission. Letter to the medical profession 1918 Oct 23. Ludvig Hekton Papers, Box 5, Folder 3, Special Collections Research Center, University of Chicago Library.
52. Illinois Influenza Commission. Letter to the medical profession 1918 Oct 24. Ludvig Hekton Papers, Box 5, Folder 3, Special Collections Research Center, University of Chicago Library.
53. Eyler JM. The fog of research: influenza vaccine trials during the 1918–19 pandemic. J Hist Med. 2009;64:401–28. [
PubMed] [
Google Scholar]
54. McCoy GW. Pitfalls in determining the prophylactic or curative value of bacterial vaccines. Public Health Rep. 1919;34:1193–5. [
Google Scholar]
55. Von Sholly AI, Park WH. Report on the prophylactic vaccination of 1536 persons against acute respiratory diseases, 1919–20. J Immunology. 1921;6:103–15. [
Google Scholar]
56. McCoy GW, Murray VB, Teeter AL. The failure of a bacterial vaccine as a prophylactic against influenza. JAMA. 1918;71:1997. [
Google Scholar]
57. A working program against influenza. Am J Public Health. 1919;9:1–13. [
PMC free article] [
PubMed] [
Google Scholar]
58. American Public Health Association. JAMA. 1918;71:2097–100. 2173–7. [
Google Scholar]
59. Prophylactic inoculation against influenza. JAMA. 1919;72:44–5. [
Google Scholar]
60. Jordan EO, Sharp WB. Effect of vaccination against influenza and some other respiratory infections. J Infect Dis. 1921;28:357–66. [
Google Scholar]
61. Winslow C-EA, Rogers JF. Statistics of the 1918 epidemic of influenza in Connecticut. J Infect Dis. 1920;26:185–216. [
Google Scholar]
62. Frost WH. The epidemiology of influenza. JAMA. 1919;73:313–38. [
Google Scholar]
63. Pearl R. On certain general statistical aspects of the 1918 epidemic in American cities. Public Health Rep. 1919;34:1743–83. [
Google Scholar]
64. Stanley LL. Influenza at San Quentin Prison, California. Public Health Rep. 1919;34:996–1008. [
Google Scholar]
65. Armstrong C. An epidemiological study of the 1920 epidemic of influenza in an isolated rural community. Public Health Rep. 1921;36:1671–702. [
Google Scholar]
66. Frost WH. Statistics of influenza morbidity with special reference to certain factors in case incidence and case fatality. Public Health Rep. 1920;35:584–97. [
Google Scholar]
67. Frost WH, Sydenstricker E. Influenza in Maryland: preliminary statistics of certain localities. Public Health Rep. 1919;34:491–504. [
Google Scholar]
68. Vaughan WT. Influenza: an epidemiological study. Baltimore: American Journal of Hygiene; 1921. p. 260. [
Google Scholar]
69. Rosenau MJ. Experiments to determine mode of spread of influenza. JAMA. 1919;73:311–3. [
Google Scholar]
70. Rosenau MJ, Keegan WJ, Goldberger J. Experiments upon volunteers to determine the cause and mode of spread of influenza, Boston, November and December, 1918. USPHS Hygienic Lab Bull. 1921;123:5–41. [
Google Scholar]
71. McCoy GW, Richey DW. Experiments upon volunteers to determine the cause and mode of spread of influenza, San Francisco, November and December, 1918. USPHS Hygienic Lab Bull. 1921;123:42–53. [
Google Scholar]
72. Rosenau MJ, Keegan WJ, Richey DW, McCoy GW, Goldberger J, Leake JP, et al. Experiments upon volunteers to determine the cause and mode of spread of influenza, Boston, February and March, 1919. USPHS Hygienic Lab Bull. 1921;123:54–99. [
Google Scholar]
73. Jordan ED. Epidemic influenza. Chicago: American Medical Association; 1927. [
Google Scholar]
Articles from Public Health Reports are provided here courtesy of
SAGE Publications




















 History tells us that the 1918 Spanish Flu killed between 50 100 million people. At the time, medical and pharmaceutical sources described it as THE MOST horrific disease process since the Black Plague of 1347, which killed an estimated 25-30 million people.
History tells us that the 1918 Spanish Flu killed between 50 100 million people. At the time, medical and pharmaceutical sources described it as THE MOST horrific disease process since the Black Plague of 1347, which killed an estimated 25-30 million people. In the book,
In the book,  Spain was neutral during WW1 and did NOT censor its press, unlike the combatting countries. As a result, Spain was the first to report the 1918 Flu epidemic and the world scapegoated Spain as the source. Thus, the Spanish Flu is born.
Spain was neutral during WW1 and did NOT censor its press, unlike the combatting countries. As a result, Spain was the first to report the 1918 Flu epidemic and the world scapegoated Spain as the source. Thus, the Spanish Flu is born.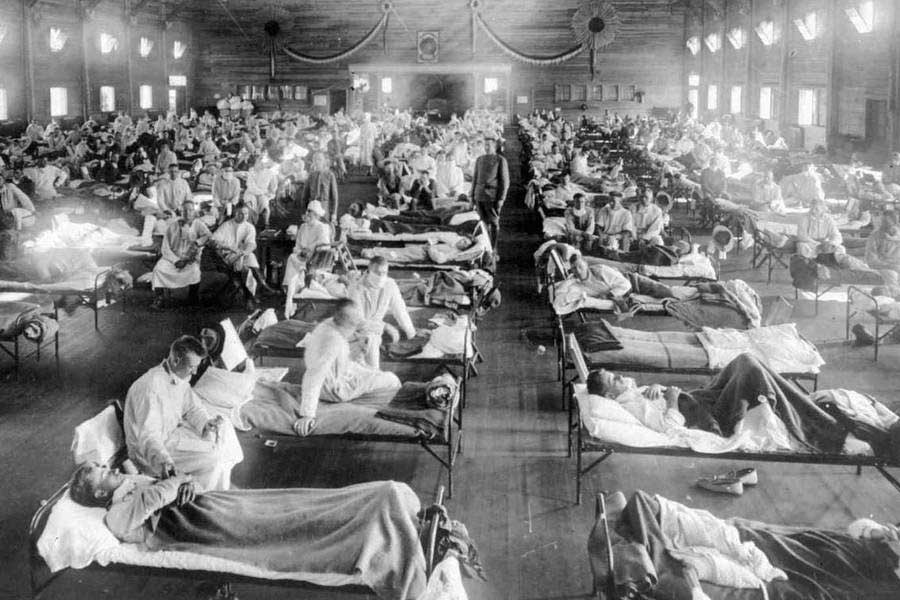 In preparation for WW1, a massive military vaccination experiment involving
In preparation for WW1, a massive military vaccination experiment involving 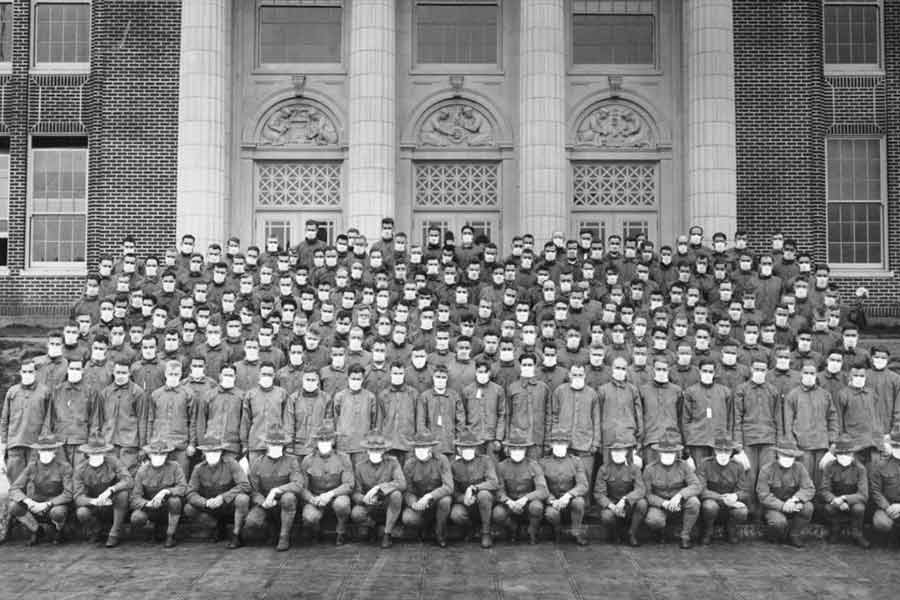 The fledgling pharmaceutical industry, sponsored by the Rockefeller Institute for Medical Research, had something they never had before a large supply of human test subjects. Supplied by the U.S. militarys first draft, the test pool of subjects ballooned to over 6 million men.
The fledgling pharmaceutical industry, sponsored by the Rockefeller Institute for Medical Research, had something they never had before a large supply of human test subjects. Supplied by the U.S. militarys first draft, the test pool of subjects ballooned to over 6 million men. Autopsies after the war proved that the 1918 flu was NOT a FLU at all. It was caused by random dosages of an experimental bacterial meningitis vaccine, which to this day, mimics flu-like symptoms. The massive, multiple assaults with additional vaccines on the unprepared immune systems of soldiers and civilians created a killing field.
Autopsies after the war proved that the 1918 flu was NOT a FLU at all. It was caused by random dosages of an experimental bacterial meningitis vaccine, which to this day, mimics flu-like symptoms. The massive, multiple assaults with additional vaccines on the unprepared immune systems of soldiers and civilians created a killing field. 



 The media, Facebook, Google, YouTube, and other privately owned communications outlets have become the self-proclaimed guardians (censors) of information.
The media, Facebook, Google, YouTube, and other privately owned communications outlets have become the self-proclaimed guardians (censors) of information. Fact Checking is often provided by paid writers from the pharmaceutical companies and not from verified, independent sources.
Fact Checking is often provided by paid writers from the pharmaceutical companies and not from verified, independent sources.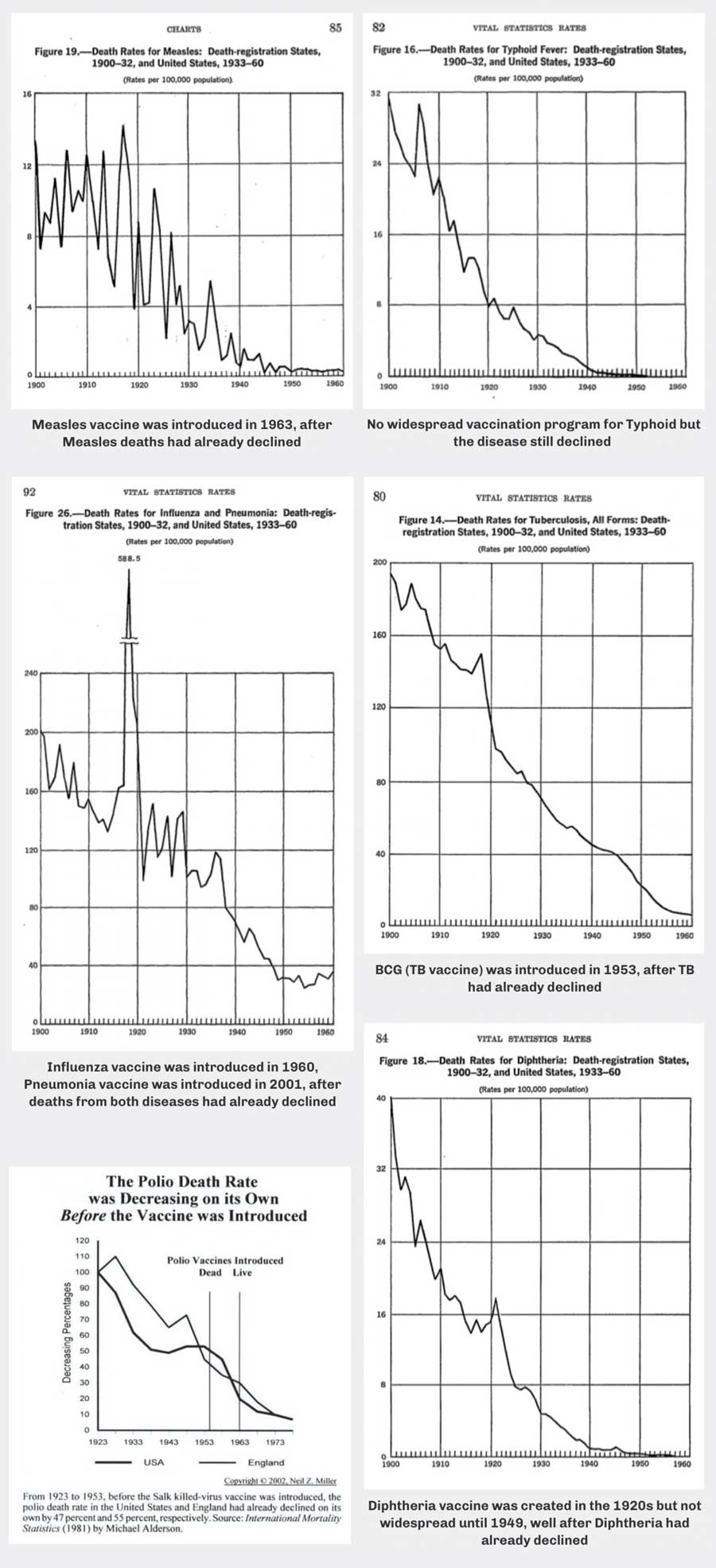 Vaccine promoters claim that vaccines wiped out most infectious diseases. History tells us a different story. The beginning of the 20th century introduced improved sanitation (sewers), water treatment plants, and vastly improved nutrition.
Vaccine promoters claim that vaccines wiped out most infectious diseases. History tells us a different story. The beginning of the 20th century introduced improved sanitation (sewers), water treatment plants, and vastly improved nutrition.